Parkinson’s Law and the Hidden Economics of Time in Audiology
Andrew Wright – Regional Director
One Source Hearing
In the middle of 2020, as COVID reshaped nearly every aspect of work, something small changed inside our company that I still think about today.
Like most organizations at the time, we had suddenly become fully dependent on virtual meetings. Days that used to involve flights, windshields, lobbies, and customer visits were replaced by back-to-back Microsoft Teams calls, where colleagues and customers lived inside tiny rectangles on a laptop screen for what felt like eight hours straight.
To help reduce fatigue, our leadership team at Sonova made a subtle adjustment to everyone’s calendars.
One-hour meetings defaulted to 50 minutes. Thirty-minute meetings defaulted to 25.
The logic was simple: give people a few minutes to collect their thoughts, grab a coffee, reply to an email, or simply step away before diving into the next virtual doom room.
At the time, it felt minor. Almost insignificant.
It’s now 2026. Most things have long since returned to the way they were before the pandemic, yet those meetings never went back to 60 and 30 minutes.
Why? Because the same amount of work somehow still gets done in 50 minutes that used to take 60.
If we’re all being honest, most meetings that once required an hour could probably fit comfortably into 40 minutes without much consequence at all.
That raises an interesting question: “If the work itself didn’t change, what exactly was the extra time doing?”
There’s a principle known as Parkinson’s Law that states:
Work expands to fill the time available for its completion.
The more time something is given, the more time it tends to consume, whether needed or not.
Once I started thinking about that concept, I couldn’t stop seeing it.
Especially inside clinics, where very different appointment types, patient needs, and economic realities are often placed into the same scheduling structure whether they should be or not.
For the past eight years, I’ve spent nearly every day working alongside small business owners across the U.S., specifically owners of privately owned audiology and hearing healthcare clinics.
Not as a product rep. Not as a clinical trainer. And not as a patient.
My vantage point has always been slightly different: sitting just outside the day-to-day operations, close enough to understand how these businesses truly function, but removed enough to view them objectively.
I don’t own these practices, nor is it lost on me that the outcomes are not mine to live with in the same way they are for the owners. I’m invited into them instead, trusted to help improve performance and support growth in what is, for many, their life’s work.
That role has taught me a lot, professionally and personally. As a dad of two young girls, I’m reminded daily that a little outside perspective can go a long way.
Perspective changes what you notice.
Different markets, different patient populations, different stages of growth, on the surface, each practice looks a little different. Over time, though, the differences start to matter less than you’d expect. The conversations become familiar. The challenges repeat themselves. Most interestingly, the way these businesses operate, especially when it comes to how time is structured, starts to look remarkably consistent.
Not necessarily for the right reasons.
Like most things inside private practices, clinic schedules tend to evolve gradually over time until nobody stops to question why they’re structured the way they are.
A sixty-minute evaluation becomes standard because that’s how it has always been scheduled. Follow-up appointments stretch because no one ever challenged whether they needed to. Small inefficiencies quietly become permanent operating structures.
The interesting part is that nothing visibly breaks.
Patients are still seen. Providers still work hard. Owners stay busy. Schedules remain full. Which is exactly why the problem persists.
One of the biggest misconceptions I see is the assumption that being fully booked means a clinic is operating at full capacity. They’re almost never the same thing.
A full schedule simply means every slot has been occupied. It provides very little context around the efficiency, structure, or intentionality behind the schedule itself.
Airport Runway Concept
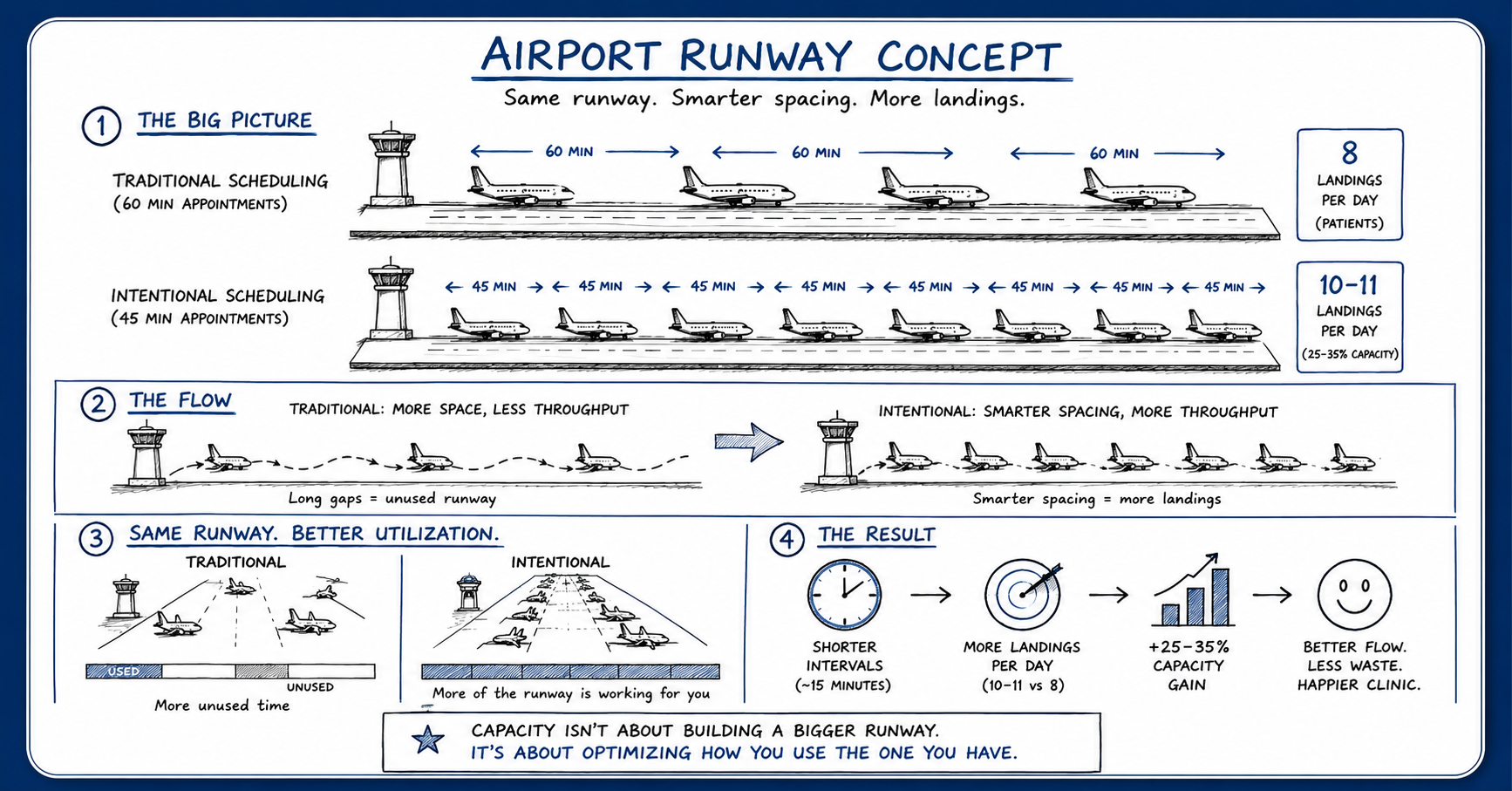
“Capacity isn’t about building a bigger runway. It’s about optimizing how you use the one you already have.”
Key Observation: The goal isn’t to rush patients or cram more appointments into a day. It’s recognizing that small structural changes in how time is allocated can quietly create meaningful increases in access, throughput, and overall clinic capacity over time.
That distinction matters more than most people realize.
Every clinic operates with a fixed amount of provider time each week. Once that time is consumed, it’s gone permanently. It cannot be stored, recovered, or replenished later. In many ways, time is the inventory. Not hearing aids. Not technology. Not even patients. Time.
The schedule is simply the mechanism used to allocate it.
That’s where Opportunity Cost quietly enters the picture.
If a fitting could reasonably be completed in 45 minutes but is routinely given 60, nothing dramatic happens in the moment. The patient still receives excellent care. The provider doesn’t feel rushed. The day moves along normally.
Economically, however, fifteen minutes disappeared.
One appointment doesn’t seem meaningful. Across an entire day, though, that excess time starts to compound. Across a week, it becomes real capacity. Across a year, it becomes meaningful revenue, patient access, and growth potential that never materialized.
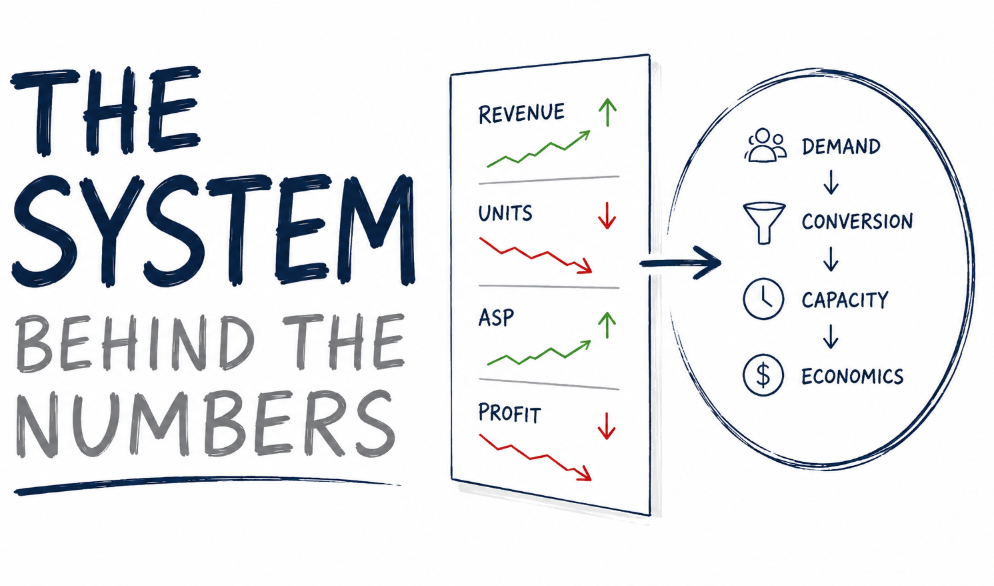
The challenge is that most clinics never see the loss directly because they rarely measure time economically.
They track revenue. Units. Conversion rates. Average selling price.
Very few measure:
• Revenue per clinical hour
• Contribution margin per hour
• Schedule utilization
• Appointment mix efficiency
Without those lenses, time feels abundant, even when it’s the single greatest constraint in the business.
That’s why the default response to growth pressure is usually predictable:
• Hire another provider
• Add one Saturday a month
• Expand hours
• Open a satellite location
Sometimes those are the right decisions.
Sometimes the existing capacity was simply never structured intentionally to begin with.
The highest-performing practices I’ve observed don’t necessarily work harder. In many cases, they’ve simply become more intentional about how time is structured, protected, and allocated.
That doesn’t mean rushing patients. It doesn’t mean stripping humanity out of care. If anything, the opposite is true. Intentional systems tend to create better experiences for both patients and providers because expectations, flow, and capacity become clearer.
What I’ve come to believe is that many practices are not constrained nearly as much by demand, staffing, competition, or even reimbursement pressure as they are by inherited operating structures they no longer question.
Especially the structures surrounding time.
The difficult part about inherited systems is that eventually they stop feeling inefficient. They just start feeling normal.
I still think about those 50-minute meetings from 2020.
Individually, ten minutes never felt meaningful. Almost nobody noticed the difference after a few weeks. Yet here we are six years later, still operating that way because the work somehow continued fitting into the smaller space.
Ten minutes at a time, over the course of six years, quietly adds up to an extraordinary amount of recovered time. Small structural changes have a way of compounding when nobody notices them day to day.
For those mathing at home, it’s north of 25 standard work weeks.
Clinic schedules aren’t much different.
Somewhere along the way, many practices accepted the same assumption most of us once accepted about 60-minute meetings:
“If the time exists, the work must require it.”

Andrew Wright – Regional Director
One Source Hearing